Taiji Miyagawa
August 13, 2024
DISCLAIMER: The views expressed in this article reflect those of the author and do no necessarily reflect the views of the Asians and Pacific Islanders for CalCare membership.
With the forces of large corporate interests driving us towards climate crisis tipping points, ongoing settler colonial genocide and increased state repression, we should nurture development of new leadership and build capacity to meet unprecedented challenges. We must enact policies in spaces that we control to protect each other.
In the face of the likelihood of simultaneous pandemics, masking requirements protect each other and promote a culture of inclusivity. Such policies within the peoples’ movement run directly counter to Democrat and Republican advocacy of mask bans and creation of new, profitable “disease markets” for corporate drug interests. We must defend the right to protect each other and it starts with enacting practices to not spread deadly airborne pathogens within our own ranks.
The Pandemic is NOT Over
The world is currently facing a SARS-CoV-2 surge once again, despite the April 2023 declaration by President Biden that the Pandemic was “over.”
As of July 2024, wastewater concentrations of COVID-19, one of the last objective means to estimate the presence of the virus in members of the population, have reached their second highest levels in history in places like San Francisco, Hawaii and elsewhere. Current data means that on average, up to approximately 1 in 33 persons are now infected.

People are still dying from the virus as more mutations arise and immunity from previous vaccination boosters wane. It is now estimated that there are over a million new cases daily in the U.S.

Vaccines help save lives, but prevent neither transmission nor infection
Vaccines have significantly reduced the incidence of death due to infection. Antibody production resulting from vaccines helps prevent cellular spread and intrusion of the virus in the body following infection, and has been shown to greatly improve one’s chances of not having to go onto a ventilator machine to assist with breathing. Some initial studies have also indicated that vaccinations may reduce one’s chances of contracting Long COVID.
However, one reason why deaths from COVID-19 continue is because immunity from the “MRNA-style” vaccines from Pfizer and Moderna declines substantially over 3 months and natural immunity from the virus seems to do the same with limited immunity especially across strain to strain. The notion of “herd immunity” for this particular virus has been proven to be both illusive and fallacy.
A big problem is that COVID-19 vaccines are not affordable to all. U.S. Government programs to make the vaccinations available and affordable to even those without insurance are helpful, but not all areas provide convenient access to pharmacies supported by these programs.
Public health leadership across the U.S. has adopted a policy of vaccines as the primary weapon against the virus. The U.S. Centers for Disease Control (CDC), Director Mandy K. Cohen in particular, consistently advocates for vaccinations, and even infamously, hand-washing, ahead of masking. In their public messaging, often, mitigation of airborne transmission, in any form, is not mentioned at all.
This is a primary reason why the pandemic continues, with no end in sight.
COVID-19 transmission occurs primarily via airborne particulates
The problem with giving mitigation of airborne transmission no better than lip-service, is that COVID-19 is, like several other deadly pathogens, transmitted primarily via aerosolized, airborne particulates during the viral incubation stage. This is also the case with other diseases such as measles, tuberculosis, and influenza (including H5N.1 bird flu), polio and monkey pox.
Vaccines do not prevent the transmission of COVID-19, nor infection.
In a closed indoor space, a single spreader can exhale, cough or sneeze enough particulates to infect multiple persons. The contaminated particulates can remain airborne for up to nine hours.
The misinformation spread by Government officials de-emphasizing the need for mitigation of transmission has led a majority of the public to forego the inconvenience of masking. Rather than move aggressively to defeat the pandemic, authorities have objectively been assisting its extension and promotion.
Conversely, study after study, despite lies promoted by far-right “anti-maskers,” confirm the effectiveness of K95/N95-grade respirators in helping to prevent spread of disease.
Most of the pubic has failed to adopt a critical stance on the government’s endangerment of the population. Beginning with the simple lie that the “pandemic is over” and all the degrees of minimizing the danger of COVID-19 as an ongoing mass, fatal and disabling event. We must take responsibility for how we have contributed to the normalization of ongoing cycles of “surges” with the arrival of each new mutation, and continued death and disablement. It didn’t need to be this way, and it need not be accepted as an irreversible situation.
It is estimated that 60% of those infected and capable of spreading COVID-19 are asymptomatic
One of the most perplexing and insidious qualities of COVID-19 has been the fact that a high percentage of infected individuals spread the virus unknowingly due to the fact of remaining asymptomatic several days into the viral incubation stage. Lack of symptoms belie the fact that such persons can be extremely contagious if steps are not taken to mitigate transmission of virus-laden aerosolized particulates.

In addition to this, false negative results of at-home rapid COVID-19 antigen tests are not uncommon. People think they are fine to mingle with others because not only are they lacking in symptoms, but may have gotten a false negative test result.
Long COVID has moved millions of people into the ranks of the disabled
One of the greatest disservices to the public by public health officials has been the dearth of education about the dangers of Long COVID. According to the World Health Organization, 10-20% of persons infected with COVID-19 contract Long COVID. However, repeated infections of COVID-19 increase one’s chances of contracting Long COVID. The estimated number of persons afflicted with Long COVID is now 400 million globally.
Long COVID is defined as a multisystem disease that have a devastating effect on any organ system, with potentially lifelong consequences. Rates of long COVID among people who have contracted SARS-CoV-2 vary controversially between studies and regions, from about 10 percent to a staggering 50 percent of people who’ve had the virus reported as having long term symptoms. – University of Nebraska Medical Center Global Center for Health Security
Much of the public remains uneducated and unaware of the dangers of Long COVID as a condition of varying degrees of disability. Many hold the misunderstanding that once vaccinated, that they are protected from both infection and Long COVID disability. While studies do exist that indicate that vaccinations diminish risk of Long COVID, there is no conclusive evidence that vaccinations prevent it.
Common symptoms included chronic fatigue, cognitive impairment, gastro-intestinal disorders. loss of taste and smell, visual impairment and assorted cardiovascular problems up to and including fatal heart attacks, even among young persons otherwise at the peak of physical conditioning such as professional athletes.
Long COVID represents the constellation of post-acute and long-term health effects caused by SARS-CoV-2 infection; it is a complex, multisystem disorder that can affect nearly every organ system and can be severely disabling. The cumulative global incidence of long COVID is around 400 million individuals, which is estimated to have an annual economic impact of approximately $1 trillion—equivalent to about 1% of the global economy. –Nature Medicine journal, August 3, 2024
Many persons have had family members and friends who seem to have recovered from COVID-19 in only 7-10 days, leading them to assume that it is no more serious than a “bad cold” or the flu. This is a dangerous misconception and leads people to engage in behaviors which increase the chances of re-infection.
The harsh reality is that if one were to contract Long COVID, there will be little to no help available and Long COVID patients simply put further strain on a system already inadequate for assisting those with disabilities. For example in Southern CA, there exist only three clinics specializing in Long COVID care. UCLA’s program has been closed for over a year and Keck Medicine’s program does not accept patients on MediCal, to the exclusion of most working class patients.
Aside from a very small number of persons, data indicates that anyone can contract Long COVID and for some, there may never be a recovery from the disabling effects of it: https://www.reuters.com/business/healthcare-pharmaceuticals/many-long-covid-patients-adjust-slim-recovery-odds-world-moves-2024-11-14/
Because there exists no “cure” for either COVID-19 nor Long COVID, it is prudent to stop spread and avoid infection. Again, vaccines do not accomplish this.
Healthcare disparities and disproportionate impacts of COVID-19
Disparities about the adverse impact of COVID-19 have been documented. The heaviest hit populations have included those with less access to healthcare, including vaccinations, medication, insurance, and education about the nature of the virus. Disparities in negative COVID-19 outcomes intersect with existing economic and class privilege and “racial” inequalities.
Some sectors of the workforce, such as lower working-class persons in the service and food-chain sectors for example, cannot afford to miss multiple weeks off of work. Many persons positioned in the lower rung of the workforce are forced to function in high-density social environments, including taking mass transit and working in high social density, indoor social interaction environments.
Cultures retaining high levels of communal interaction, including some Native Indian tribes or Pacific Islanders groups have suffered disproportionately.
Limited access to healthcare services for many, and exorbitant drug pricing are a fundamental characteristic of the present U.S. healthcare system. For example, one of the most effective “drug cocktails” for reducing viral load in the body to reduce spread and long term entrenchment and replication of the virus following infection, Paxlovid, which includes antiviral drugs used for the treatment of AIDS, is affordable for most with insurance coverage.
For the uninsured, most of whom are working class and immigrant, the retail cost of Paxlovid is over $1600. Persons without insurance number over 2.5 million in CA and over 25 million nationally.

Some people are more vulnerable to the negative effects of SARS-CoV-2 than others. Among the most vulnerable are persons with already-compromised immune systems such as people fending off major diseases such as cancer. Obesity and conditions like high blood pressure can make one more susceptible to Long COVID disablement. Persons living and working in crowded environments such as incarcerated individuals or seniors in nursing homes are at higher risk. If one is already on a respirator device, they are not able to wear common K95/N95 masks for self-protection.
The most cost effective way to reduce transmission for those able to do so is by use of higher-grade masks, or respirators, with filtration material that trap microscopic infected aerosolized airborne particulates. These include well-fitted NIOSH standard K95 and N95 respirators. Cloth masks and loose-fitting surgical masks have limited effectiveness. The more persons masking, the lower the number of deadly virus particulates circulating in the air.

Proper ventilation and filtration of the air will also reduce the density of particulates in a given environment. HEPA grade filtration, including low-cost Corsi-Rosenthal filtration and UV light filtration technologies are prudent in densely-populated environments. Utilizing air quality measurement technology is also a good practice.
Mask requirements serve the people and the movement for social change
Masking requirements and the above clean air quality measures protect everyone, but particularly those with disproportionate vulnerability to deadly airborne pathogens. Mask requirements and clean air practices are integral to countering the existing dominant economic/political/cultural system which places less value on persons with disabilities, persons of non-European decent and persons with less economic privilege due to lower incomes.
A growing number of Long COVID activists assess that the CDC and other Federal and regional Public Health agencies are under control of private corporate interests, the same ones that finance political career campaigns of 95-plus% of politicians via campaign contributions and 24/7 political lobbying of elected officials. The healthcare infrastructure itself is also dominated by privately-operated, for-profit hospitals that have no interests in implementing air filtration infrastructure upgrades or increasing budgets for quality staff personal protection equipment (PPE). These expenses are viewed as negatively impacting “bottom-line” earnings reports. Measures to help provide for patient safety are not deemed “profitable” by for-profit enterprise. Public health officials are appointed by politicians who reach positions of power due to cozy relationships with such monied interests.


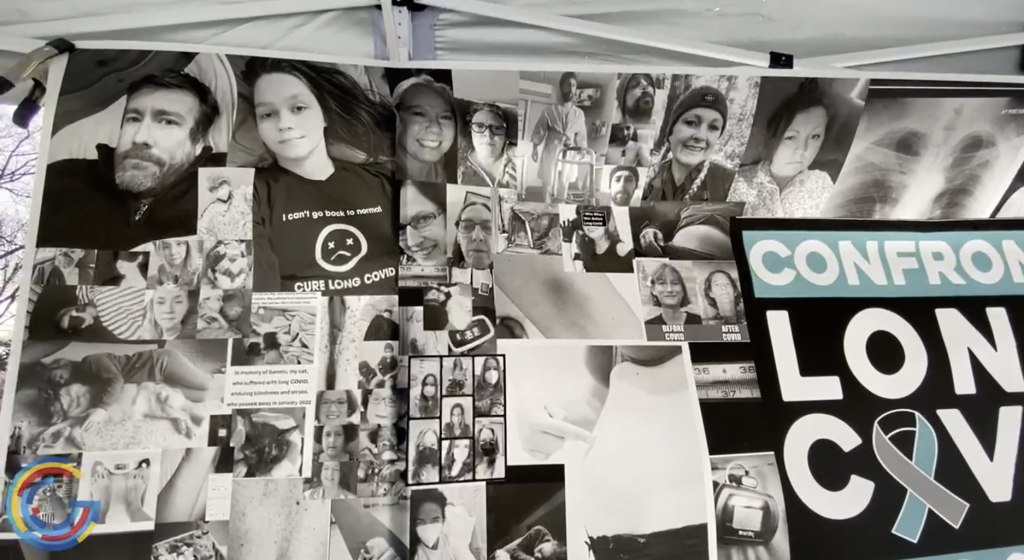
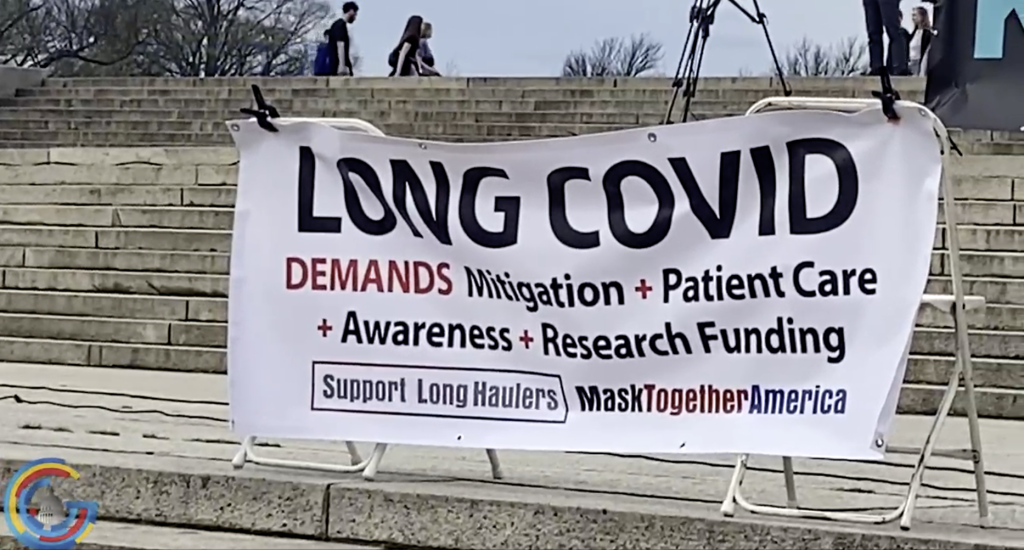
(Above: March 15, 2024 activists in Washington DC calling for increased research and patient care for Long COVID patients. Photos from wdbj7.com)
On a broader social level, the hypocrisy of far-right conservatives in politicizing masking as an infringement upon “personal freedoms” has been thoroughly exposed by their support for fascistic mask bans in North Carolina and Nassau County, NY. Under these laws, the public no longer has legal freedom to protect themselves or each other from inhalation and exhalation of deadly airborne pathogens. We must stand up to actively oppose these mask bans. It shouldn’t be the Long COVID and disabled community bearing the burden of this fight alone.
Beyond the Long COVID community, more than a few healthcare reform advocates suspect that monopolistic pharmaceutical corporations view COVID-19 as an new opportunity for massive profits. Disease, under the current healthcare system, is a vehicle for wealth extraction from the economy, in the same way that the current society de-emphasizes preventative healthcare in general. For these private interests there is no short-term motivation for actually defeating SARS-CoV-2. Therefore, policies to decrease spread and reduce rates of mutation are not pursued in earnest.
Lack of mask requirement policies in spaces we control are objectively consistent with current capitalistic, profit-motivated policy to downplay the critical need for mitigation of airborne transmission of COVID-19 and other deadly airborne pathogens.
Keep each other safe, embrace the humanity of all

There is no good reason for progressive-minded activists to tail the harmful policy-crafting of the corrupt elected political leadership and appointed public health officials. These policies, following the declared “end” to the pandemic have now been extended into laws and proposals for banning the wearing of masks in public. Mask requirements are not even being implemented in most healthcare facilities anymore, making them extremely high-risk environments for contracting airborne diseases.
Rather than being lax about reducing airborne transmission of airborne diseases, we should be fighting for policies that protect the public health interests and be holding public officials accountable to that cause, not private-profit interests. Currently, the only people doing this nationally are the COVID-aware community, Long COVID patients and other members of the broader disabled communities. And many who are now forced to avoid healthcare facilities due to unsafe mask and clean air practices.
Mask requirements should be viewed as a lowest-level type of mutual aid activity. As part of our ongoing efforts to transform society, we should engage in promoting a culture of caring for one another. We should strive to do our best to keep each other safe. We should value all lives, not just those of persons deemed to have “able bodies” alone. Persons with disabilities rely upon the compassion of others to allow for their participation in society. Advocacy of masking and requiring of masking at events, and exercising clean air practices should be central to this effort.
Mask requirements are the only true pro-working-class and pro-oppressed peoples policy. A “masks recommended” or “masks optional” policy capitulates to the privileged deemed to be “able-bodied,” who have better access to medical care. Such policies dismissing the dangers of COVID-19 discriminates against those with existing disabilities and immune-compromised status. At minimum, failure to implement mask requirements reflects a poor understanding of the nature of currently circulating harmful airborne pathogens, which now include the H5N.1 bird flu virus and Monkey Pox (MPox).
The predominant “survival of the fittest” and “everyone for themselves” mindset of capitalist economy is integral to human life being valued relative only to the function of persons as part of a surplus and reserve exploitable labor pool. The notion that certain lives are expendable simply because they do not serve profit is inhumane.
Viewing things such as air filtration, ventilation and masking to accommodate disabled persons as burdensome is consistent with the idea that only “able-bodied” people should be allowed to participate in social change movement work.
In reality, the failure to implement harm-reduction practices with respect to transmission of deadly airborne pathogens is analogous to not engaging in language justice practices, but while the latter can be more challenging to implement (i.e, shortages of skilled live event translators, and multilingual headset equipment), K95-grade masking and Corsi Rosenthal filtering are relatively inexpensive.
We should strive to envision a new society that is inclusive and respectful of all working and oppressed peoples. One that does not discriminate because of physical disability. While it is true that this is not always easy or even practical to do so in every instance, we should nurture such aspirations as best we can nonetheless.
At the most basic level, we should strive to promote a culture of caring and keep each other safe. Implementing mask requirements during a pandemic is the least we can do.
Take Action
- Implement mask requirements, especially for indoor events, but be aware that transmission does occur outdoors as well, especially without social distancing.
- Deploy effective air ventilation and filtration practices.
- Donate K95/N95 masks to local community organizations
- Donate low-cost Corsi Rosenthal filters to local community organizations and schools
- Help push public policy leftward to offset prioritization of private-profit interests. E.g. tell Presidential candidate Kamala Harris to address mitigation of airborne transmission of COVID-19. https://www.whitehouse.gov/contact/vicepresident/
- Join the COVID-aware and disabled community efforts to stop mask bans already implemented in North Carolina and Nassau County, NY, but also under proposal elsewhere in New York in addition to Nassau County, in Los Angeles, Philadelphia (currently, ski masks) and Chicago.
https://peoplescdc.org/2024/06/18/no-mask-bans/ - Support the efforts to validate Bio-markers for Long COVID: https://www.gofundme.com/f/your-support-is-needed-for-the-long-covid-foundation